
Children grow in ways that can be difficult to interpret, even for experienced parents. A toddler who seems chubby may slim down naturally as they become more active. A child who appears slim may be growing perfectly healthily. And a child whose weight seems unremarkable on observation may, when measured and plotted carefully, be following a trajectory that warrants clinical attention.
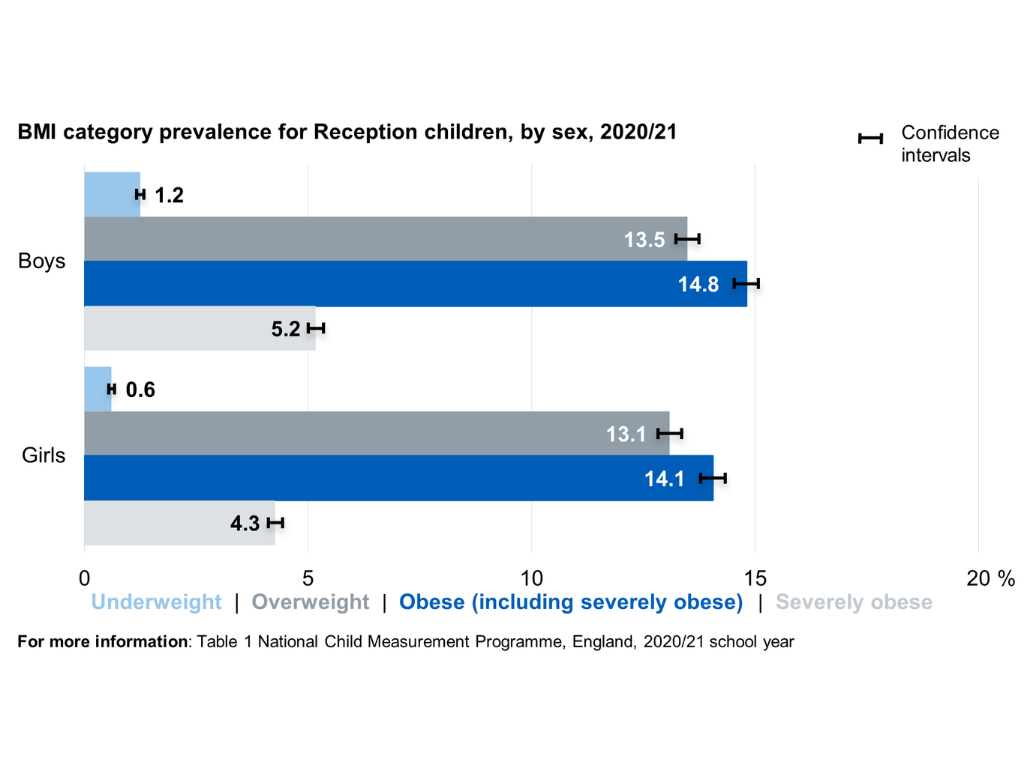
But there might always be a level of worry. After all, childhood obesity is a significant and growing public health concern in the UK. According to the National Child Measurement Programme, in 2022 to 2023, 22.7% of children in reception year and 37.8% of children in year six were living with overweight or obesity [1].
These figures represent not only a health challenge in childhood itself but a strong predictor of health outcomes in adult life, given the well-established tracking of obesity and its associated cardiometabolic risk factors from childhood into adulthood [2]. Though it is rarely straight forward, not every child who carries a little extra weight is on a concerning trajectory; it is important that families are not unnecessarily alarmed by normal variations in childhood growth patterns.
The distinction between normal development and early obesity requires careful clinical assessment, and this is where specialist input can make a meaningful difference.

How Children Grow And Gain Weight
Growth in childhood is not a smooth, linear process. It is characterised by periods of rapid changes interspersed with plateaus, and the pattern varies considerably between individual children depending on genetic, nutritional, hormonal and environmental factors [3].
In the first two years of life, growth is rapid and weight gain is expected and healthy. Most children roughly triple their birth weight by twelve months and continue to gain weight steadily through early childhood [4].
During this period, a degree of visible chubbiness is entirely normal and reflects the laying down of subcutaneous fat that supports brain development, immune function and thermoregulation in infancy.
Between the ages of two and five, growth typically slows and many children naturally slim down as they become more mobile and their appetite adjusts to their slower rate of growth. Parents who are accustomed to the rapid weight gain of infancy sometimes become concerned during this phase, interpreting the slowing of weight gain as a problem when it is in fact entirely expected [5].
The primary school years, roughly ages five to ten, are characterised by steady, relatively predictable growth, during which weight and height increase in parallel and the body mass index typically remains relatively stable [3]. It is during this period, however, that the early signs of excess weight gain often become apparent, and when intervention, if needed, is most likely to be effective.
Puberty introduces another period of rapid and variable change. The pubertal growth spurt produces significant increases in both height and weight, with the timing and magnitude of these changes varying considerably between individuals [6]. Girls typically enter puberty earlier than boys, and the associated changes in body composition, including increases in fat mass that are normal and hormonally driven, can sometimes be misinterpreted as problematic weight gain.
What Body Mass Index Tells Us and What It Does Not
Body mass index (BMI), calculated as weight in kilograms divided by the square of height in metres, is the most widely used screening tool for assessing weight status in children as well as adults [7]. In children, however, BMI must be interpreted in the context of age and sex, because normal body fat levels change considerably across childhood and differ between boys and girls, particularly around puberty.
For this reason, childhood BMI is expressed as a centile relative to a reference population rather than as a raw number, using growth reference charts, such as the UK90 charts used by the NHS [7].
A child at the 85th to 94th centile for BMI is classified as overweight, meaning their BMI is higher than 85% of their peers. A child at or above the 95th centile is classified as obese [8].
It is important to understand that BMI centile is a screening tool rather than a diagnostic instrument. A child with a high BMI centile may have a large muscle mass rather than excess fat, and a child with a BMI in the normal range may still have an unfavourable body composition if muscle mass is low and fat mass is disproportionately high [9]. This is why clinical assessment goes beyond BMI alone to consider the child’s growth trajectory over time, their physical development, their dietary patterns and activity levels, and any associated symptoms or risk factors that might indicate a metabolic or endocrine contributor to weight gain.
Normal Weight Variation vs Early Signs of Obesity
The distinction between normal variation in childhood weight and the early stages of a concerning weight trajectory is not always immediately obvious, and it requires a degree of clinical nuance that goes beyond a single measurement.
Normal weight variation in childhood is characterised by weight:
- That tracks reasonably consistently along a centile channel over time,
- Is proportionate to height gain,
- Is not associated with symptoms of metabolic dysfunction or significant lifestyle factors that would drive excess weight gain [3][5].
A child who is at the 75th centile for weight and the 70th centile for height, whose weight has been in this range consistently, and who is otherwise well and active, is following a normal growth pattern even if they look somewhat heavier than some of their peers.
On the other hand, early signs of obesity typically involve weight gain that is crossing centile channels upwards over time, a divergence between weight centile and height centile such that weight is considerably higher than height relative to the reference population, and often a pattern of dietary and activity behaviours that provide a clear environmental explanation [10].
Specific early signs that may warrant a professional assessment include:
- A BMI centile consistently at or above the 91st centile, particularly if it has risen over time
- Weight gain that appears disproportionate to the child’s height and developmental stage
- A family history of obesity-related conditions, including type two diabetes, cardiovascular disease or metabolic syndrome
- Signs of insulin resistance, such as acanthosis nigricans, a darkening and thickening of the skin in the neck folds and armpits
Symptoms that might indicate an underlying hormonal or genetic cause of weight gain, including short stature, delayed or early puberty, fatigue or learning difficulties [11][12].
It is also important to be alert to the psychological dimension of childhood weight concerns. Children who are overweight are at significantly higher risk of experiencing bullying, low self-esteem and body image difficulties, and these psychosocial consequences can themselves drive the emotional eating and reduced physical activity that perpetuate weight gain [13]. A compassionate, non-judgmental approach to assessment and support is essential, focusing on health and well-being rather than weight as a number.
The Role of Genetics and Environment
Weight in children, as in adults, reflects the interaction of genetic predisposition with environmental factors, and understanding both is important in making sense of an individual child’s weight trajectory. Genetic factors account for a significant proportion of the variation in childhood BMI, with studies of twins estimating heritability of obesity at between 40% and 70% [14].
Children with two obese parents have a significantly higher risk of developing obesity than those without a family history, and this risk reflects both shared genetic factors and shared environmental patterns around food and activity. However, genetic predisposition is not destiny. The dramatic increase in childhood obesity rates over recent decades cannot be explained by changes in genetics alone, and reflects instead the profound shift in the food environment, physical activity patterns and sedentary behaviour that characterises modern childhood in high-income countries [15].
Ultra-processed food consumption, increased screen time, reduced active play, and the increasing convenience and availability of energy-dense foods have collectively created an environment in which weight gain is the path of least resistance for children with a genetic susceptibility. Understanding this interaction helps to frame the conversation around childhood weight in a way that is constructive rather than blame-attributing.
When to Seek a Specialist Assessment
A specialist assessment for childhood weight concerns is appropriate in several circumstances, and seeking one earlier rather than later is consistently associated with better outcomes. If your child’s weight centile has been rising consistently over time, if their BMI is consistently above the 91st centile, or if you have noticed signs that might suggest an underlying medical cause of weight gain, a thorough clinical assessment is the right next step [11].
Similarly, if dietary changes and increased activity have not produced the expected results, or if your child is experiencing the psychosocial consequences of weight concerns, including bullying, low mood or disordered eating behaviours, specialist input can provide both clinical clarity and practical, tailored support.
A comprehensive assessment in a specialist setting goes considerably beyond what a standard GP appointment can provide. It includes:
- A detailed growth history plotted on appropriate charts
- A thorough clinical examination including:
- Assessment for signs of metabolic dysfunction
- A review of dietary patterns and activity levels
- Screening for underlying endocrine or genetic causes where clinically indicated
- The development of a personalised, family-centred management plan that is realistic, evidence-based and compassionate in its approach [16].
In fact, research published in the International Journal of Obesity found that children who received structured, multidisciplinary intervention for obesity at an early stage of weight gain achieved significantly better outcomes in terms of BMI trajectory, cardiometabolic risk factors and psychological well-being compared with those who received standard care or no intervention [17].
Paediatric Weight Assessment at The Health Suite Leicester
At our Paediatric Weight Management Clinic in The Health Suite Leicester, we support children and young people in reaching a healthier weight in a compassionate, family-focused environment.
We understand that weight management is complex. Every child is unique, and their care should be too. That’s why we create personalised healthcare plans that not only focus on physical health, but also nurture confidence, social life, and emotional wellbeing.
We offer expert-led, family-centred care that combines medical assessment, nutritional guidance, and emotional support to help children build healthier habits and long-term confidence.
Book a paediatric weight assessment today at The Health Suite Leicester.
References:
- NI Direct. Early or delayed puberty. Available at: https://www.nidirect.gov.uk/conditions/early-or-delayed-puberty
- NHS. Early or delayed puberty. Available at: https://www.nhs.uk/conditions/early-or-delayed-puberty/
- Bräuner EV, et al. Trends in the Incidence of Central Precocious Puberty and Normal Variant Puberty Among Children in Denmark, 1998 to 2017. JAMA Netw Open. 2020; 1;3(10):e2015665
- Breehl L, Caban O. Physiology, Puberty. [Updated 2023 Mar 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available at: https://www.ncbi.nlm.nih.gov/books/NBK534827/
- YourHormones.info. Hormones in puberty. Available at: https://www.yourhormones.info/explore/discover/hormones-in-puberty/
- Healthychildren.org. Physical Development in Girls: What to Expect During Puberty. Available at: https://www.healthychildren.org/English/ages-stages/gradeschool/puberty/Pages/Physical-Development-Girls-What-to-Expect.aspx?utm_source=perplexity
- Lee HS. Why should we be concerned about early menarche? Clin Exp Pediatr. 2021;64(1):26-27
- Sharma L, Daley SF. Precocious Puberty. [Updated 2025 Nov 7]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available at: https://www.ncbi.nlm.nih.gov/books/NBK544313/?
- Whincup PH, et al. Age of menarche in contemporary British teenagers: survey of girls born between 1982 and 1986. BMJ. 2001;5;322(7294):1095-6
- Golding J, et al. Measures of puberty in the Avon Longitudinal Study of Parents and Children (ALSPAC) offspring cohort [version 1; peer review: 3 approved with reservations]. Wellcome Open Res. 2023, 8:453
- Joshua A. Bell, et al. Influence of puberty timing on adiposity and cardiometabolic traits: A Mendelian randomisation study. PLoS Med. 2018; 28;15(8):e1002641
- Mendle J, et al. Understanding Puberty and Its Measurement: Ideas for Research in a New Generation. J Res Adolesc. 2019;29(1):82-95
- Joinson C, et al. Early Menarche and Depressive Symptoms From Adolescence to Young Adulthood in a UK Cohort. Journal of the American Academy of Child & Adolescent Psychiatry. 2013; 52;6: 591-598.e2
- Mendolia S, et al. Early puberty in 11-year-old girls: Millennium Cohort Study findings. Arch Dis Child. 2016;101(10):950-956
- Emmanuel M, Bokor BR. Tanner Stages. [Updated 2022 Dec 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available at: https://www.ncbi.nlm.nih.gov/books/NBK470280/?
- NHS. Guideline for Investigation of early (precocious) and late (delayed) puberty in girls and boys. Available at: https://www.nn.nhs.scot/speg/wp-content/uploads/sites/36/2024/03/NSD610-016.19-SPEG-Precocious-Delayed-Puberty.pdf
- NHS. Precocious Puberty: Advice for Referrers. Available at: https://www.clinicalguidelines.scot.nhs.uk/rhc-for-health-professionals/guidelines/primary-care-referral-guidelines/medical-paediatric-pre-referral-guidance/precocious-puberty-advice-for-referrers/
- Cho JH, Jung HW, Shim KS. Growth plate closure and therapeutic interventions. Clin Exp Pediatr. 2024;67(11):553-559
- Shim KS. Pubertal growth and epiphyseal fusion. Ann Pediatr Endocrinol Metab. 2015;20(1):8-12
- Jean‐Claude C, et al. Precocious puberty and statural growth. Human Reproduction Update. 2004; 10:2: 135-147
- Joinson C, et al. Early menarche is associated with an increased risk for depressive symptoms in adolescent girls in a UK cohort. Journal of E and C Health. 2009; 63;2
- Joinson C, et al. Early Menarche and Depressive Symptoms From Adolescence to Young Adulthood in a UK Cohort. Journal of American Academy of Child & Adolescent Psychiatry. 2013; 52;6: 591-598
- Alghamdi A. Precocious Puberty: Types, Pathogenesis and Updated Management. Cureus. 2023 Oct 22;15(10):e47485
- Brix N, et al. Childhood overweight and obesity and timing of puberty in boys and girls: cohort and sibling-matched analyses. Int J Epidemiol. 2020;1;49(3):834-844
- NHS. The LHRH test. Available at: https://www.swbh.nhs.uk/wp-content/uploads/2023/12/The-LHRH-test-ML5183.pdf
- NHS. LHRH Stimulation Test. Available at: https://leaflets.ekhuft.nhs.uk/lhrh-stimulation-test/html/