
Anal fissures are a notably painful condition, and yet they are also one of the most underreported. The combination of an intimate location, discomfort and a degree of social stigma means that many people endure months or even years of pain before seeking help. For some, it does. Acute anal fissures, those that have been present for less than six weeks, heal spontaneously in the majority of cases with conservative management including dietary changes, increased fluid intake and topical treatments [1].
But for those whose fissure persists beyond six weeks and becomes chronic, the picture is different. Chronic anal fissures are considerably less likely to resolve without intervention, and the cycle of pain, spasm and impaired healing that sustains them tends to worsen rather than improve without targeted treatment [2].
Botulinum toxin injection, more widely known by the brand name Botox, has emerged over the past two decades as one of the most effective, evidence-based treatments for chronic anal fissure, offering high rates of healing with minimal risk and a rapid return to normal daily life. Understanding how it works, who it is suitable for and what the evidence shows is the first step for anyone who has been living with this condition and wondering whether there is a better option available to them.
Understanding Chronic Anal Fissures
An anal fissure is a small tear in the lining of the anal canal, typically occurring at the posterior midline and producing pain, bleeding and spasm during and after bowel movements [3]. The pain is often described as severe, sharp or burning, and can persist for hours after defecation, making everyday activities, including sitting, walking and working, deeply uncomfortable.
The condition is more common than many people realise. It affects individuals of all ages and both sexes, with a particular prevalence in young and middle-aged adults, and is among the most frequent reasons for referral to colorectal surgical services [4]. In women, it is also a recognised consequence of childbirth, with obstetric trauma representing a significant risk factor for fissure development [5].
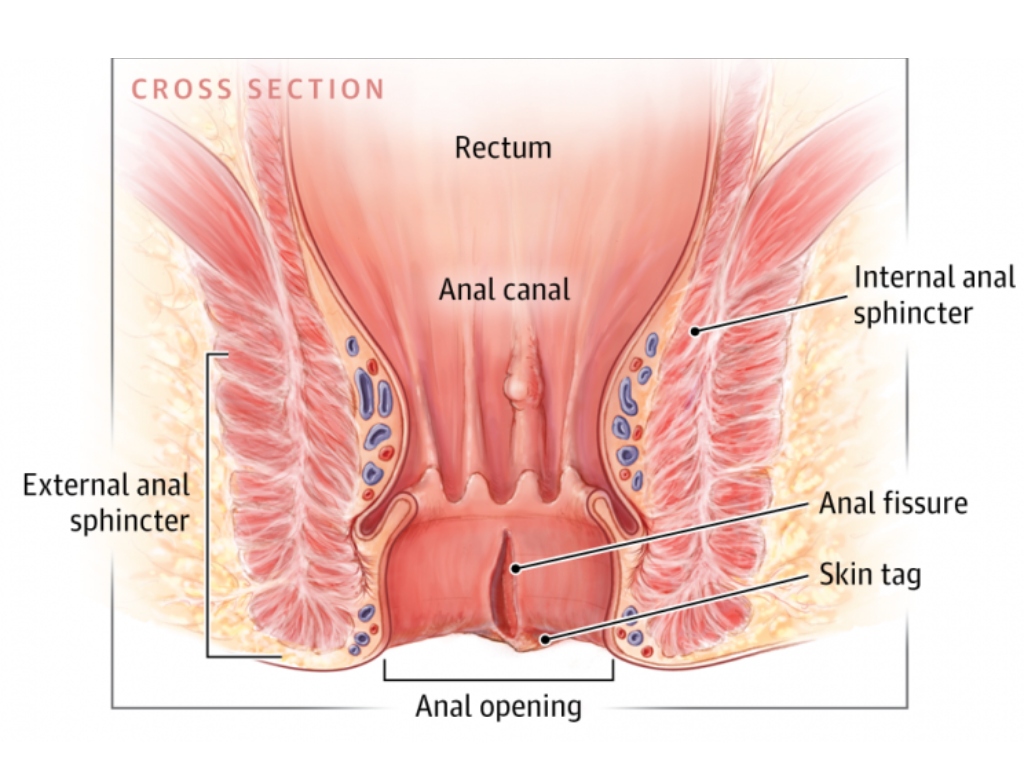
The mechanism that converts an acute fissure into a chronic one is well understood. The pain of a fissure triggers a reflexive spasm of the internal anal sphincter, the involuntary muscle that maintains resting anal tone. This spasm reduces blood flow to the anoderm, the specialised skin lining the anal canal, impairing the tissue’s ability to heal.
The reduced blood flow prevents the tissue from healing, which prolongs the pain, which keeps the muscle in spasm, creating a cycle that the body simply cannot break on its own [6]. In a chronic fissure, this cycle has become established. The fissure typically develops characteristic features, including a sentinel pile at its lower margin, hypertrophied anal papillae at its upper margin, and exposed internal sphincter fibres at its base, all of which indicate that spontaneous healing is unlikely [2][7].
Why Conservative Treatment Often Falls Short
For acute fissures, conservative measures including increased dietary fibre, adequate hydration, sitz (salt) baths and topical anaesthetics are effective first-line management and should always be tried first [1]. For chronic fissures, these measures address symptoms without tackling the underlying sphincter spasm that is preventing healing, which is why they so frequently provide only partial or temporary relief.
Topical pharmacological treatments, most commonly glyceryl trinitrate (GTN) ointment and topical calcium channel blockers such as diltiazem, work by chemically relaxing the internal anal sphincter, thereby reducing spasm and improving anodermal blood flow [8]. Both are recommended in NICE guidelines as first-line pharmacological treatment for chronic anal fissure, and both can be effective [9].
However, GTN is associated with significant rates of headache, which limits its tolerability for many patients, and both topical treatments require consistent application over an extended period, with recurrence rates following discontinuation that remain a clinical concern [8][10]. Diltiazem cream often is restricted within NHS practice due to its high prescription costs, especially within primary care prescribing.
Surgical sphincterotomy, which involves dividing a portion of the internal anal sphincter to relieve spasm permanently, has historically been regarded as the gold standard treatment for chronic anal fissure refractory to medical management, with healing rates consistently above 90% in published series [11]. However, it carries a small but clinically meaningful risk of faecal incontinence, reported in studies at rates ranging from 1% to 8% depending on the extent of sphincter division and patient factors, which has led both clinicians and patients to seek alternatives with a more favourable safety profile [12].
How Botox Works as a Treatment
Botox is a neurotoxin produced by the bacterium Clostridium botulinum that works by blocking the release of acetylcholine at the neuromuscular junction, thereby preventing muscle contraction [13]. When injected into the internal anal sphincter, it produces a temporary, controlled reduction in sphincter tone that lasts for approximately three to four months, during which time the reduced spasm allows blood flow to the area to enhance recovery and allow the fissure to heal [6][14].
The effect is reversible. As the Botox is metabolised, normal sphincter function gradually returns, which is why the risk of permanent incontinence associated with surgical sphincterotomy does not apply to Botox injections. [12][15].
This reversibility is one of the most clinically important features of the treatment and the primary reason it has become the preferred intervention for many colorectal specialists managing chronic anal fissure. The procedure itself is typically performed as an outpatient procedure under local anaesthetic, takes a matter of minutes, and requires no hospital admission or significant recovery period. Most patients are able to return to normal activities the same day or within 24 hours [16].
What the Evidence Shows
The evidence base for Botox in chronic anal fissure has grown substantially over the past two decades and is now sufficiently robust to support its use as a recommended treatment option in international colorectal guidelines [3]. A landmark randomised controlled trial published in the New England Journal of Medicine compared botulinum toxin injection with placebo in patients with chronic anal fissure and found that 73% of those receiving Botox achieved complete healing at two months, compared with 13% in the placebo group [17].
Additionally, a systematic review and meta-analysis published in Diseases of the Colon and Rectum found that Botox injection produced healing rates of between 60% and 80% in patients with chronic anal fissure, with low rates of adverse effects and no significant risk of permanent incontinence [18]. Additionally, a Cochrane review examining all surgical and pharmacological treatments for chronic anal fissure concluded that Botox injection represented the best balance of efficacy and safety among the available options, and recommended it as the treatment of choice for patients where topical therapy has failed [10][19].
What to Expect from Treatment
For patients considering Botox injection for chronic anal fissure, understanding what the treatment involves and what to expect in terms of recovery and outcomes is important. The procedure begins with a clinical assessment to confirm the diagnosis, assess fissure chronicity, exclude other anorectal pathology and discuss treatment options in full.
Where Botox injection is agreed as the appropriate treatment, it is performed under local anaesthetic in an outpatient setting. The injection is administered at one or more sites into the internal anal sphincter on either side of the fissure – a process that takes only a few minutes and produces minimal discomfort beyond that of the local anaesthetic injection itself [16][20].
Most patients notice a reduction in sphincter spasm and associated pain within the first one to two weeks following injection. Fissure healing typically occurs over the following six to twelve weeks, with most patients achieving complete resolution within three months [17][21].
Follow-up assessment at six to eight weeks allows healing to be confirmed and any further management to be planned if needed. Patients are typically advised on dietary and lifestyle measures to reduce the risk of recurrence, including adequate fibre intake, hydration and stool-softening strategies where appropriate [1][20].
Chronic Anal Fissure Treatment at The Health Suite Leicester
If you have been living with the pain of a chronic anal fissure and have not found lasting relief from topical treatments, a specialist assessment can establish whether botulinum toxin injection is the right next step for you. At The Health Suite Leicester, our colorectal specialists have extensive experience in the assessment and treatment of chronic anal fissure.
We provide a thorough clinical evaluation, a clear explanation of all available treatment options, and, where botulinum toxin injection is indicated, a straightforward outpatient procedure with prompt follow-up to monitor your recovery. Living with chronic anal fissure pain is not something you have to accept. Effective, minimally invasive treatment is available, and the evidence for its benefit is clear.
Book your consultation at The Health Suite Leicester for lasting relief today.
References:
- Mapel DW, et al. The epidemiology and treatment of anal fissures in a population-based cohort. BMC Gastroenterol. 2014;14:129
- Brisinda G, et al. Chronic anal fissure: pathophysiology, diagnosis and treatment. Ann Ital Chir. 2012;83(4):287–300
- Stewart DB, et al. Clinical practice guideline for the management of anal fissures. Dis Colon Rectum. 2017;60(1):7–14
- Farouk R, et al. Sustained internal sphincter hypertonia in patients with chronic anal fissure. Dis Colon Rectum. 1994;37(5):424–429
- Corby H, et al. Anal canal pressures are low in women with postobstetric anal fissure. Br J Surg. 1997;84(1):86–88
- Schouten WR, et al. Ischaemic nature of anal fissure. Br J Surg. 1996;83(1):63–65
- Lund JN, Scholefield JH. Aetiology and treatment of anal fissure. Br J Surg. 1996;83(10):1335–1344
- Carapeti EA, et al. Randomised controlled trial shows that glyceryl trinitrate heals anal fissures, higher doses are not more effective, and there is a high recurrence rate. Gut. 1999;44(5):727–730
- NICE. Anal Fissure. Clinical Knowledge Summary. London: NICE; 2023. Available at: https://bnf.nice.org.uk/treatment-summaries/anal-fissure/
- Nelson RL, et al. Non surgical therapy for anal fissure. Cochrane Database Syst Rev. 2012;(2):CD003431
- Littlejohn DR, Newstead GL. Tailored lateral sphincterotomy for anal fissure. Dis Colon Rectum. 1997;40(12):1439–1442
- Breivik S, et al. Risk of anal incontinence after lateral internal sphincterotomy for anal fissure: a systematic review and meta-analysis. Colorectal Dis. 2021;23(6):1311–1321
- Simpson LL. Molecular pharmacology of botulinum toxin and tetanus toxin. Annu Rev Pharmacol Toxicol. 1986;26:427–453
- Jost WH, Schimrigk K. Use of botulinum toxin in anal fissure. Dis Colon Rectum. 1993;36(10):974
- Nasr M, et al. Botulinum toxin versus surgery in the treatment of chronic anal fissure. J Gastrointest Surg. 2010;14(1):150–154
- Colak T, et al. Comparison of procedures in treatment of chronic anal fissure: a prospective randomised study. Acta Chir Belg. 2003;103(6):607–611
- Brisinda G, et al. A comparison of injections of botulinum toxin and topical nitroglycerin ointment for the treatment of chronic anal fissure. N Engl J Med. 1999;341(2):65–69
- Sajid MS, et al. Botulinum toxin versus surgical sphincterotomy for the treatment of chronic anal fissure: a systematic review and meta-analysis. Dis Colon Rectum. 2008;51(12):1899–1906
- Nelson RL, et al. Operative procedures for fissure in ano. Cochrane Database Syst Rev. 2011;(11):CD002199
- Maria G, et al. Influence of botulinum toxin site of injections on healing rate in patients with chronic anal fissure. Am J Surg. 2000;179(1):46–50
- Brisinda G, et al. Botulinum neurotoxin to treat chronic anal fissure: results of a randomised controlled trial. Aliment Pharmacol Ther. 2016;44(7):704–710