
There is something particularly frustrating about a frozen shoulder. It does not stop you in your tracks all at once. It takes things from you gradually, a little more reach here, a little more comfort there, until one day you realise you cannot lift your arm above your shoulder, sleep through the night, or get dressed without planning around it.
Frozen shoulder, known as adhesive capsulitis, is a condition characterised by progressive pain and stiffness in the shoulder joint caused by inflammation and thickening of the connective tissue envelope that surrounds and stabilises the shoulder [1]. It affects approximately 2–5% of the general population and up to 20% of people with diabetes, and while it can resolve on its own over time, that process typically takes between two and four years and is associated with significant pain, disability and reduced quality of life throughout [2][3].
For people who cannot afford to wait years for a gradual natural resolution, and for those whose symptoms are not improving on their own, hydrodilatation offers a well-evidenced, minimally invasive treatment option that can accelerate recovery, restore movement and significantly reduce pain. Understanding what the procedure involves, what the evidence shows and who is most likely to benefit is the starting point for anyone weighing their options.
Understanding Frozen Shoulder and Who It Affects
The shoulder is the most mobile joint in the human body, capable of movement across a wide range of planes and directions.
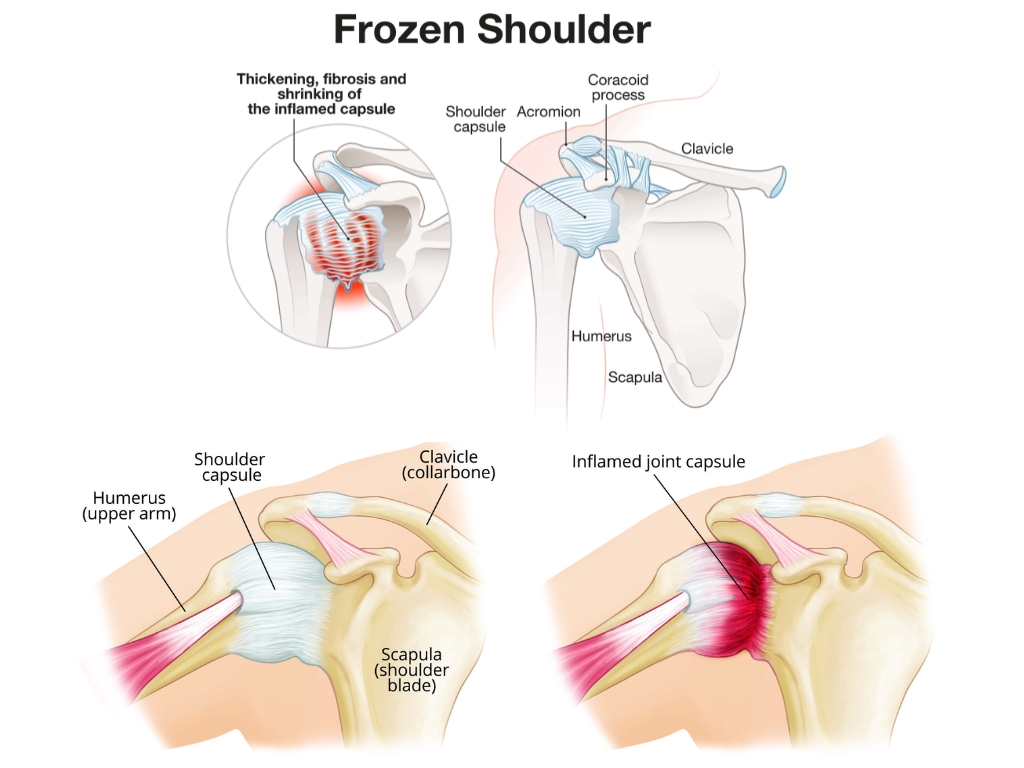
That mobility depends on the integrity and flexibility of the joint capsule, a fibrous sleeve of connective tissue that encloses the glenohumeral joint and normally allows a generous range of movement [4].
In adhesive capsulitis, the joint capsule becomes inflamed, thickened and contracted. The volume of the joint space reduces significantly, sometimes to as little as 5–6ml compared with a normal capacity of around 25–30ml, and the synovial fluid that lubricates the joint diminishes [5]. The result is a shoulder that is increasingly reluctant to move, stiff in all planes of motion rather than in one direction only, and often acutely painful at the end range of whatever movement remains.
The condition typically progresses through three overlapping phases.
- The freezing phase is dominated by pain, often severe and frequently worse at night, with progressively worsening stiffness developing over weeks to months [6].
- The frozen phase sees pain begin to ease, but stiffness reaches its maximum, with range of motion substantially reduced across all planes.
- The thawing phase involves a gradual, often slow, return of movement as the capsule loosens over time [6][7].
The cause of adhesive capsulitis is not fully understood, but it is more common in women than men, most frequently presents between the ages of 40 and 60, and has a well-established association with diabetes mellitus, thyroid dysfunction, cardiovascular disease and prolonged immobility following shoulder injury or surgery [2][8]. People with diabetes are not only at higher risk of developing frozen shoulder but tend to experience a more severe course and a slower recovery, making early intervention particularly important in this group [2][3].
Why Waiting Is Not Always the Answer
The conventional advice that frozen shoulder will eventually resolve on its own is technically accurate for many patients, but it obscures the scale of what waiting actually involves. Studies looking at patients managed conservatively have reported that full recovery can take anywhere from one to four years, and that a meaningful proportion of patients continue to experience some residual stiffness or pain beyond that period [9].
During the intervening months and years, frozen shoulder has a significant burden on daily life. Disrupted sleep is among the most commonly reported consequences, with many patients unable to lie on the affected side or find any comfortable sleeping position during the freezing and frozen phases [6]. Occupational impact is also considerable, with research published in the Journal of Shoulder and Elbow Surgery finding that frozen shoulder was associated with significant work absence and reduced productivity, particularly in roles requiring overhead activity or manual dexterity [10].
For people with diabetes, the case for active intervention rather than watchful waiting is particularly strong. A systematic review published in Diabetes Care found that diabetic patients with frozen shoulder had significantly longer recovery times, greater functional limitation and poorer outcomes with conservative management compared to non-diabetic patients, and were more likely to require procedural intervention to achieve satisfactory recovery [3][8]. The question for most patients is therefore not whether they should seek treatment, but which treatment is most likely to deliver meaningful improvement in the shortest time with the least risk.
What Is Hydrodilatation
Hydrodilatation, also known as distension arthrography or hydrodistension, is a minimally invasive procedure that treats frozen shoulder by injecting a carefully controlled volume of fluid, typically a combination of saline, corticosteroid and local anaesthetic, directly into the shoulder joint capsule under imaging guidance [11]. The fluid distends the contracted capsule, stretching and in some cases rupturing the fibrous adhesions that have formed within it, thereby increasing joint volume and restoring range of motion [5][11].
The corticosteroid component reduces inflammation within the joint, while the local anaesthetic provides immediate pain relief and makes the procedure well-tolerated. The entire procedure is performed under ultrasound or fluoroscopic guidance to ensure precise needle placement and accurate fluid delivery into the joint space [12]. The procedure is performed as an outpatient treatment, typically takes between 15 and 30 minutes, and requires no general anaesthetic or hospital admission.
Most patients can return home shortly afterwards and are encouraged to begin gentle mobilisation exercises the same day to capitalise on the increased joint volume achieved during the procedure [13].
What the Evidence Shows
The evidence base for hydrodilatation in frozen shoulder is well established and continues to grow, with multiple randomised controlled trials and systematic reviews supporting its efficacy across all phases of the condition. A landmark randomised controlled trial published in the British Medical Journal compared hydrodilatation with placebo injection in patients with frozen shoulder and found that those receiving hydrodilatation demonstrated significantly greater improvements in pain, range of motion and shoulder function at six weeks and at six months, with the benefits maintained at long-term follow-up [14].
Additionally, a systematic review and meta-analysis published in the British Journal of Sports Medicine found that hydrodilatation combined with corticosteroid produced significantly greater improvements in pain and function compared with corticosteroid injection alone, physiotherapy alone or placebo [15]. In fact, a Cochrane review of interventions for frozen shoulder concluded that hydrodilatation with corticosteroid provided clinically meaningful short-term improvements in pain and function, and recommended it as an effective treatment option for patients who had not achieved adequate relief from initial conservative management [16].
A prospective study published in Skeletal Radiology found that ultrasound-guided hydrodilatation produced successful capsular distension in over 90% of procedures, with significant improvements in range of motion observed at four weeks in the majority of patients, and that outcomes were further improved when the procedure was combined with a structured physiotherapy programme commencing shortly after the injection [12][15].
Who Is Most Likely to Benefit
Hydrodilatation is most effective when performed at the right stage of the condition and in appropriately selected patients.
Treatment is considered when a patient:
- Has a confirmed diagnosis of adhesive capsulitis
- Has experienced symptoms for at least six to eight weeks
- Has not achieved adequate relief from initial conservative management including physiotherapy, oral anti-inflammatory medication and standard corticosteroid injection [11][13].
Patients in the freezing and early frozen phases tend to achieve the best outcomes, as the capsule at this stage retains sufficient elasticity to respond well to distension [6][15]. That said, patients in the frozen phase can also benefit meaningfully, particularly where pain and stiffness are significantly affecting daily function and sleep. People with diabetes represent a group in whom hydrodilatation has particular value, given the poorer outcomes associated with conservative management in this population and the evidence supporting procedural intervention as a more reliable route to recovery [3][8].
Patients who have previously undergone corticosteroid injection alone without achieving adequate improvement may also find that hydrodilatation delivers the additional mechanical benefit needed to restore movement. Hydrodilatation is generally not recommended as a first-line treatment before conservative measures have been tried, and is not appropriate in patients with active shoulder infection, recent shoulder surgery or certain structural abnormalities that would be better addressed through alternative means [11]. A thorough clinical assessment before the procedure is essential to confirm the diagnosis, exclude other causes of shoulder pain and stiffness, and ensure the treatment plan is appropriately tailored to the individual.
What to Expect from Treatment
For patients considering hydrodilatation, understanding what the experience involves from assessment through to recovery helps to manage expectations and prepare for the process. The clinical assessment prior to the procedure will include a detailed history of symptoms, physical examination of the shoulder and a review of any relevant imaging. Where the diagnosis of adhesive capsulitis is confirmed and hydrodilatation is agreed as an appropriate treatment, the procedure is scheduled as an outpatient appointment [1][11].
On the day, the shoulder is prepared and local anaesthetic is administered into the skin and underlying tissue before the needle is introduced into the joint space under ultrasound guidance. The fluid mixture is then injected slowly into the joint. Patients typically feel a sensation of pressure and stretch during the injection as the capsule distends, which can be briefly uncomfortable but is well tolerated by the majority [12][13].
Most patients notice some immediate improvement in range of motion following the procedure, reflecting the mechanical effect of capsular distension. Pain levels in the first 24 to 48 hours may temporarily increase as the joint responds to the procedure, before improving as the corticosteroid takes effect over the following days [13][15]. Physiotherapy commencing within a few days of the procedure plays an important role in consolidating and extending the gains in range of motion achieved through hydrodilatation. Research has consistently shown that outcomes are significantly better when the procedure is followed by a structured, progressive exercise programme compared with hydrodilatation alone [15]. Patients are typically reviewed at four to six weeks to assess progress and determine whether any further treatment is needed.
Frozen Shoulder Treatment at The Health Suite Leicester
If your shoulder has been limiting your life for weeks or months, and conservative measures have not delivered the improvement you were hoping for, a specialist assessment can establish whether hydrodilatation is the right treatment for you.
At The Health Suite Leicester, our musculoskeletal specialists provide consultant-led assessment and ultrasound-guided hydrodilatation for frozen shoulder, with a thorough clinical evaluation beforehand to confirm the diagnosis and ensure the treatment plan is right for your individual circumstances.
Through this, we can help to:
- Reduce capsular restriction
- Improve range of movement
- Make physiotherapy and stretching more effective.
Every patient receives clear guidance on what to expect before, during and after the procedure, and a structured follow-up plan to support recovery. Frozen shoulder is a condition that responds well to the right intervention at the right time. The sooner it is treated, the sooner life gets back to normal.
Book your assessment and start restoring shoulder movement today.
Similar Treatment for Frozen Shoulder at The Health Suite
References:
- Mapel DW, et al. The epidemiology and treatment of anal fissures in a population-based cohort. BMC Gastroenterol. 2014;14:129
- Brisinda G, et al. Chronic anal fissure: pathophysiology, diagnosis and treatment. Ann Ital Chir. 2012;83(4):287–300
- Stewart DB, et al. Clinical practice guideline for the management of anal fissures. Dis Colon Rectum. 2017;60(1):7–14
- Farouk R, et al. Sustained internal sphincter hypertonia in patients with chronic anal fissure. Dis Colon Rectum. 1994;37(5):424–429
- Corby H, et al. Anal canal pressures are low in women with postobstetric anal fissure. Br J Surg. 1997;84(1):86–88
- Schouten WR, et al. Ischaemic nature of anal fissure. Br J Surg. 1996;83(1):63–65
- Lund JN, Scholefield JH. Aetiology and treatment of anal fissure. Br J Surg. 1996;83(10):1335–1344
- Carapeti EA, et al. Randomised controlled trial shows that glyceryl trinitrate heals anal fissures, higher doses are not more effective, and there is a high recurrence rate. Gut. 1999;44(5):727–730
- NICE. Anal Fissure. Clinical Knowledge Summary. London: NICE; 2023. Available at: https://bnf.nice.org.uk/treatment-summaries/anal-fissure/
- Nelson RL, et al. Non surgical therapy for anal fissure. Cochrane Database Syst Rev. 2012;(2):CD003431
- Littlejohn DR, Newstead GL. Tailored lateral sphincterotomy for anal fissure. Dis Colon Rectum. 1997;40(12):1439–1442
- Breivik S, et al. Risk of anal incontinence after lateral internal sphincterotomy for anal fissure: a systematic review and meta-analysis. Colorectal Dis. 2021;23(6):1311–1321
- Simpson LL. Molecular pharmacology of botulinum toxin and tetanus toxin. Annu Rev Pharmacol Toxicol. 1986;26:427–453
- Jost WH, Schimrigk K. Use of botulinum toxin in anal fissure. Dis Colon Rectum. 1993;36(10):974
- Nasr M, et al. Botulinum toxin versus surgery in the treatment of chronic anal fissure. J Gastrointest Surg. 2010;14(1):150–154
- Colak T, et al. Comparison of procedures in treatment of chronic anal fissure: a prospective randomised study. Acta Chir Belg. 2003;103(6):607–611
- Brisinda G, et al. A comparison of injections of botulinum toxin and topical nitroglycerin ointment for the treatment of chronic anal fissure. N Engl J Med. 1999;341(2):65–69
- Sajid MS, et al. Botulinum toxin versus surgical sphincterotomy for the treatment of chronic anal fissure: a systematic review and meta-analysis. Dis Colon Rectum. 2008;51(12):1899–1906
- Nelson RL, et al. Operative procedures for fissure in ano. Cochrane Database Syst Rev. 2011;(11):CD002199
- Maria G, et al. Influence of botulinum toxin site of injections on healing rate in patients with chronic anal fissure. Am J Surg. 2000;179(1):46–50
- Brisinda G, et al. Botulinum neurotoxin to treat chronic anal fissure: results of a randomised controlled trial. Aliment Pharmacol Ther. 2016;44(7):704–710