
Laser Treatment for Pilonidal Sinus: A Minimally Invasive Option
A pilonidal sinus is a condition that many people have never heard of until they develop one, at which point it tends to become difficult to think about much else.
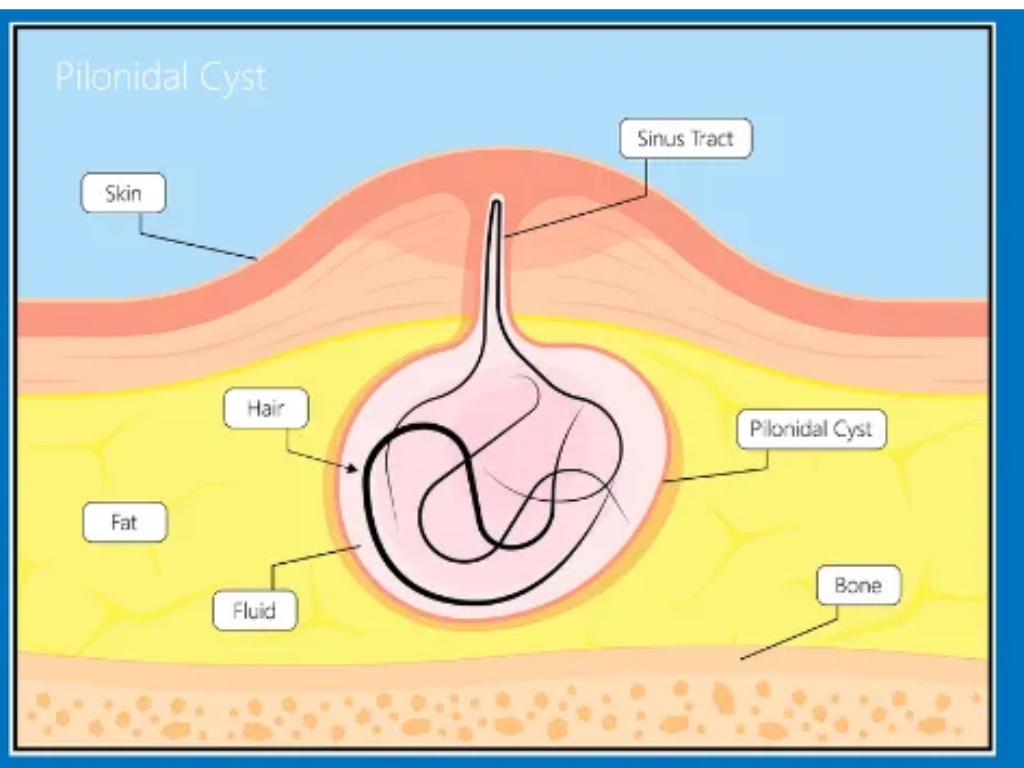
The pain of an acute abscess, the disruption to sitting, working and everyday activity, and the anxiety about what treatment might involve can all make pilonidal sinus disease a significant source of distress, particularly for the young adults it most commonly affects. Pilonidal sinus disease is a chronic condition affecting the skin at the top of the buttock crease, near the tailbone, in which one or more small tunnels or cavities form beneath the skin, typically containing hair, debris and inflammatory tissue.1
It most commonly affects young adults, those who sit for long periods, and people with coarse or thicker body hair or a deep natal cleft, and it has a well-established association with friction and sweating in the area.2 The condition has a well-deserved reputation for being difficult to treat definitively. Traditional surgical approaches, while effective in many cases, involve significant wounds in an anatomically challenging location, prolonged recovery, and recurrence rates that remain a clinical problem even after apparently successful surgery.3
For many patients, the prospect of conventional surgery, with weeks of wound care, restricted activity and time off work, is a significant barrier to seeking treatment. But laser-assisted pilonidal sinus treatment, known as PiLAC, Pilonidal Laser-Assisted Closure, offers a minimally invasive alternative to traditional open surgery in appropriately selected cases.
Understanding what the procedure involves, what the evidence shows and who is most likely to benefit is the starting point for anyone exploring their options.
-
Pilonidal Sinus Disease Explained
The word pilonidal comes from the Latin for nest of hair, a description that reflects the characteristic finding of hair within the sinus tracts that develop in the natal cleft.1
The current consensus supports an acquired rather than congenital origin, with loose hair from the surrounding skin being drawn into the natal cleft by suction forces created by movement, penetrating the skin and triggering a foreign body inflammatory reaction that leads to tract formation.5
Symptoms of pilonidal sinus disease include pain and swelling near the tailbone, recurrent abscess formation, persistent or intermittent discharge, and discomfort when sitting or exercising.6
Without definitive treatment, chronic pilonidal sinus disease rarely resolves spontaneously. The tracts become progressively more complex over time, with branching and lateral extension increasing the surgical challenge if and when intervention eventually becomes necessary.7
Early treatment, before the disease has become extensive, consistently produces better outcomes across all treatment modalities.
The condition typically presents in one of two ways. An acute pilonidal abscess presents suddenly with pain, swelling, redness and discharge in the natal cleft, and requires prompt drainage to relieve the acute episode before definitive treatment can be planned.
Chronic pilonidal sinus disease presents as one or more persistent openings in the natal cleft skin, which may discharge intermittently, cause recurrent episodes of inflammation and abscess, and produce chronic discomfort that significantly affects sitting, activity and quality of life.6
Why Traditional Surgery Has Limitations
Conventional surgical treatment for pilonidal sinus involves excision of the sinus tracts and the surrounding tissue, either leaving the wound open to heal by secondary intention or closing it primarily or with a flap reconstruction.3 Each approach has merits and limitations, but all share certain features that make the treatment experience challenging for patients.
Open excision, in which the wound is left open and packed to heal from the base upwards, produces reliable eradication of disease but requires wound care that typically continues for six to twelve weeks, during which time sitting is uncomfortable, activity is restricted and time off work is often necessary.8 Recurrence rates following open excision range from 10% to 30% in published series, reflecting the difficulty of completely eradicating the disease in an anatomically challenging and mechanically loaded site.3,8
Primary closure techniques reduce healing time but are associated with higher rates of wound breakdown and infection in the natal cleft, where the opposing skin surfaces create a warm, moist environment that is prone to wound complications.9 Flap-based reconstructions, including the Karydakis and Limberg flap procedures, produce better outcomes than simple primary closure by moving the wound away from the midline, but they involve more extensive surgery and carry their own complication profiles.10
The common thread is that conventional surgery, however well performed, involves a meaningful recovery burden and a recurrence rate that remains a genuine clinical concern. These limitations have driven considerable interest in less invasive approaches that can achieve durable healing with a significantly better patient experience.
What PiLAC Involves
PiLAC is a minimally invasive procedure that uses laser energy delivered directly into the sinus tracts to destroy the tract lining, eliminate the contained hair and debris, and stimulate the closure and healing of the cavity from within, without the need for wide excision or significant external wounds.4
The procedure aims to minimise tissue removal, reduce wound size, shorten recovery time and reduce post-operative discomfort compared with conventional surgical approaches. A radial laser fibre is introduced into each sinus tract, and laser energy is delivered along the length of the tract as the fibre is withdrawn, producing controlled thermal destruction of the epithelial lining and the hair-containing contents of the sinus.11
The pit openings on the skin surface are treated to remove the entry points through which hair penetrates, and the treated tracts are left to heal from within without the need for packing or open wound management. Many cases can be performed as a day case, often under local anaesthetic, depending on clinical assessment.12 Patients can usually return to normal activities within a few days rather than the weeks required following conventional surgery, and the absence of a large open wound in the natal cleft eliminates the most burdensome aspect of conventional postoperative recovery.
It is important to note that if an acute abscess is present at the time of assessment, drainage will typically be needed first before PiLAC can be performed as definitive treatment. Treating the acute episode first allows the inflammation to settle and gives the laser treatment the best chance of achieving complete and durable healing.
What Can PiLAC Treat
PiLAC may be considered for patients with chronic pilonidal sinus disease, recurrent disease following previous treatment, persistent discharge that has not settled with conservative measures, and symptoms that are significantly affecting daily life and activity. 4, 11
The procedure is most effective in patients with primary or moderately complex pilonidal sinus disease. Patients whose disease has become highly complex, with multiple branching tracts, extensive lateral extension or large abscess cavities, may require conventional surgical management to achieve complete eradication.
A thorough clinical assessment is essential to determine the most appropriate approach for each individual.7
What the Evidence Shows
The evidence base for laser treatment of pilonidal sinus has grown substantially over the past decade, with multiple prospective studies and comparative series now available to inform clinical decision-making. A prospective study published in Techniques in Coloproctology examining laser-assisted sinus closure in patients with chronic pilonidal sinus disease found primary healing rates of 87% at one year, with a median return to normal activity of three days and a low rate of complications.11
The authors noted that the procedure was particularly well-suited to patients with uncomplicated or moderately complex disease who wished to avoid the recovery burden of conventional surgery.11 A multicentre study published in Colorectal Disease comparing laser treatment with conventional surgical approaches found that laser-treated patients had significantly shorter operative times, significantly faster return to work and daily activity, and lower rates of postoperative pain and wound complications, with healing rates comparable to those achieved with open excision at twelve-month follow-up. 14
Additionally, a systematic review examining minimally invasive techniques for pilonidal sinus disease found that these approaches consistently produced faster recovery, lower complication rates and comparable healing rates to conventional surgery, while being associated with significantly higher patient satisfaction scores.15 The review concluded that minimally invasive techniques should be considered as first-line treatment for suitable patients with pilonidal sinus disease, particularly those with primary or recurrent uncomplicated disease.15
For recurrent pilonidal sinus following previous conventional surgery, laser treatment offers a particularly valuable option. Re-excision of recurrent disease in a previously operated field is technically more demanding and carries higher complication rates than primary surgery, making a minimally invasive approach that avoids further wide excision especially attractive in this setting.4,14
Pilonidal Sinus Assessment and PiLAC Treatment at The Health Suite Leicester
If you have been living with pilonidal sinus disease and have been putting off seeking treatment because of concerns about surgery, recovery time or time away from work, PiLAC may offer the solution you have been looking for.
At The Health Suite Leicester, we provide a thorough clinical assessment to establish the anatomy and complexity of your sinus disease, discuss all available treatment options, and, where PiLAC is appropriate, offer a straightforward day case procedure designed to get you back to normal life as quickly as possible.
Pilonidal sinus disease is a genuinely treatable condition, and with the right approach, most patients achieve durable healing without the prolonged recovery that has historically made treatment so disruptive.
Minimally Invasive Pilonidal Sinus Treatment
Find out more about PiLAC laser treatment for pilonidal sinus at The Health Suite Leicester and book your consultation today

Pilonidal Sinus Laser Treatment
Private Pilonidal Sinus Laser Treatment in Leicester. Minimally invasive PiLAC closure for chronic tracts, promoting fast, packing-free recovery.
References
- Patey DH, Scarff RW. Pathology of postanal pilonidal sinus: its bearing on treatment. Lancet. 1946;2(6428):484–486
- Doll D, et al. Time and rate of sinus formation in pilonidal sinus disease. ANZ J Surg. 2008;78(6):540–543
- Al-Khamis A, et al. Healing by primary versus secondary intention after surgical treatment for pilonidal sinus. Cochrane Database Syst Rev. 2010;(1):CD006213
- Dessily M, et al. Pilonidal sinus laser treatment: a prospective cohort study. Colorectal Dis. 2017;19(4):370–375
- Bascom J, Bascom T. Failed pilonidal surgery: new paradigm and new operation leading to cures. Arch Surg. 2002;137(10):1146–1150
- McCallum IJ, King PM, Bruce J. Healing by primary closure versus open healing after surgery for pilonidal sinus. BMJ. 2008;336(7649):868–871
- Stauffer VK, et al. Common surgical procedures in pilonidal sinus disease: a meta-analysis, merged data analysis, and review on recurrence. Sci Rep. 2018;8(1):3058
- Enriquez-Navascues JM, et al. Meta-analysis of randomised controlled trials comparing different techniques with primary closure for chronic pilonidal sinus. Tech Coloproctol. 2014;18(10):863–872
- Solla JA, Rothenberger DA. Chronic pilonidal disease: an assessment of 150 cases. Dis Colon Rectum. 1990;33(9):758–761
- Akca T, et al. Prospective randomised trial comparing modified Karydakis flap versus modified Limberg flap for the treatment of sacrococcygeal pilonidal sinus. Ann Surg. 2016;263(2):266–270
- Milone M, et al. New minimally invasive treatment of pilonidal sinus with laser: one-year follow-up results. Tech Coloproctol. 2017;21(5):363–366
- Pappas AF, Christodoulou DK. A new minimally invasive treatment of pilonidal sinus disease. Tech Coloproctol. 2018;22(12):919–922
- Meinero P, et al. Endoscopic pilonidal sinus treatment (EPSiT) in recurrent pilonidal disease: a prospective international multicentre study. Colorectal Dis. 2016;18(8):835–840
- Dessily M, et al. Laser treatment versus wide surgical excision for pilonidal sinus disease. Colorectal Dis. 2019;21(7):798–803
- Ghnnam WM, et al. Minimally invasive procedures for pilonidal disease: a systematic review. Surg Innov. 2020;27(4):420–430
Have a query about Laser Treatment for Pilonidal Sinus: A Minimally Invasive Option?
We recognise that getting the healthcare assistance you need can be difficult. So if you have a query, feel free to contact us and one of our treatment co-ordinators will be happy to help. We aim to reply to all queries within 24 hours (Mon – Fri).