
Haemorrhoid Banding vs Surgery: Why Patients Prefer Minimally Invasive Treatment
Haemorrhoids are one of the most common conditions seen in colorectal practice, and yet they remain one of the most under-discussed. Many people manage symptoms for months or years before seeking help. This can be because individuals feel embarrassed to raise the subject and because they assume the treatment will be worse than the problem.
Equally, a reluctance to seek help may simply reflect a lack of awareness that effective, minimally invasive treatment options are available – often requiring no general anaesthetic, no hospital admission and no significant recovery period. In the UK, it is estimated that around one in three people will experience symptomatic haemorrhoids at some point in their lives, with bleeding, prolapse, itching, discomfort and hygiene difficulty among the most commonly reported symptoms. 1
Despite this prevalence, haemorrhoids are frequently undertreated, with many people relying on over-the-counter creams and dietary changes that address symptoms without resolving the underlying problem. For patients with internal haemorrhoids of grade one to three, rubber band ligation (RBL), more commonly known as haemorrhoid banding, has become the most widely performed outpatient procedure in colorectal practice, offering high rates of symptom resolution with minimal discomfort, no anaesthetic and a rapid return to normal activity. 2
Understanding how banding compares with surgical haemorrhoidectomy, what each procedure involves, and why the evidence consistently supports banding as the preferred first-line intervention for most patients is the foundation for an informed treatment decision.
-
The Challenge of Haemorrhoids Explained
Haemorrhoids are cushions of vascular tissue within the anal canal that play a normal and important role in continence, contributing to fine control of gas and liquid stool alongside the sphincter muscles. 3
They become a clinical problem when they enlarge, prolapse or bleed, typically as a result of increased pressure within the anal canal from straining, constipation, prolonged sitting, pregnancy or other contributing factors.
Internal haemorrhoids develop above the dentate line, the anatomical boundary within the anal canal above which there are no somatic pain receptors, which is why they do not typically cause pain unless they prolapse and become irreducible or thrombosed. 3, 4
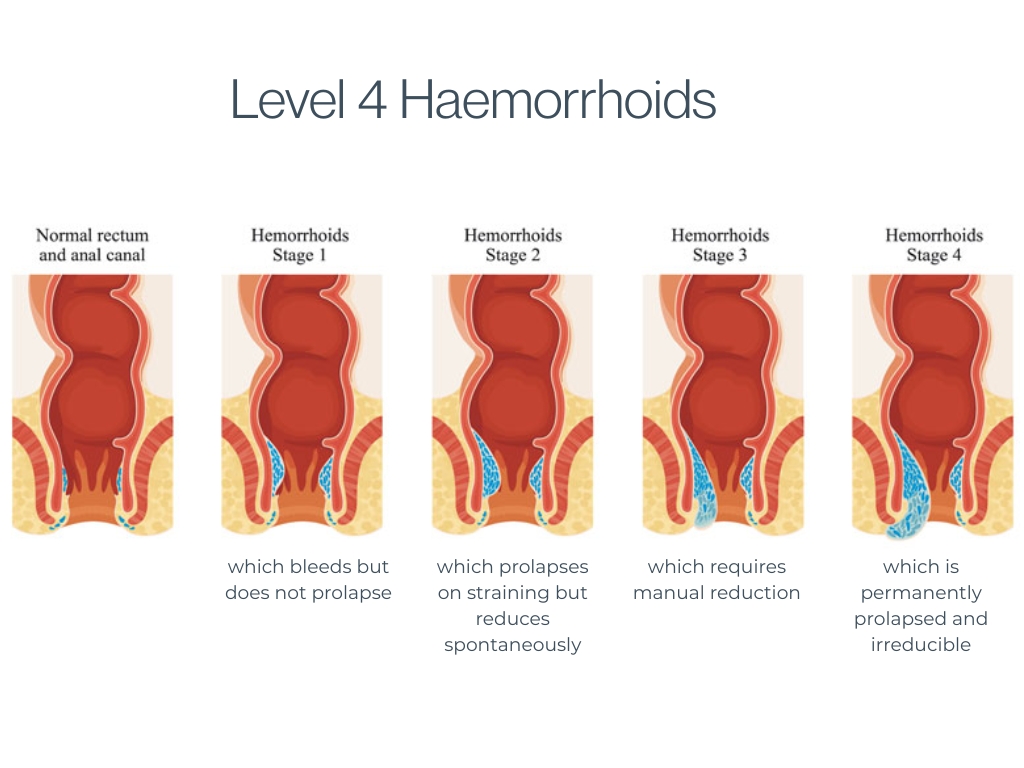
They are classified by degree of prolapse on a four-grade scale:
- Grade one, which bleeds but does not prolapse,
- Grade two, which prolapses on straining but reduces spontaneously,
- Grade three, which requires manual reduction,
- Grade four, which is permanently prolapsed and irreducible. 4
External haemorrhoids develop below the dentate line in the skin-lined portion of the anal canal and lower anal verge, and because this area is richly innervated with somatic pain receptors, they can be acutely and severely painful, particularly when they thrombose. 3
Understanding this distinction matters because treatment options and their appropriateness differ depending on the type and grade of haemorrhoid present, and an accurate clinical assessment is the necessary starting point for any treatment decision.
What Haemorrhoid RBL Involves
RBL is a procedure in which small elastic bands are applied to the base of internal haemorrhoidal tissue above the dentate line, cutting off the blood supply to the haemorrhoid. 5
The banded tissue undergoes ischaemic necrosis over the following days, falls off, and the resulting small wound heals with fibrosis, preventing further prolapse. The procedure is performed in an outpatient setting using a proctoscope and a banding device, takes 20-30 minutes, and because the bands are applied above the dentate line in the insensate portion of the anal canal, it is well tolerated without anaesthetic in the vast majority of patients. 5,6
Most people experience a sensation of fullness or mild discomfort in the hours following the procedure, which typically settles with simple pain relief, and are able to return to normal activities the same day or the following day. Multiple haemorrhoids can be treated over a course of banding sessions, typically scheduled four to six weeks apart to allow healing between treatments.
A systematic review published in the British Journal of Surgery found that most patients required two to three banding sessions to achieve complete symptom resolution, with high rates of satisfaction and low rates of serious complications. 6
What Surgical Haemorrhoidectomy Involves
Surgical haemorrhoidectomy involves the excision of haemorrhoidal tissue under general or spinal anaesthetic, and remains the most effective treatment for large grade three and grade four haemorrhoids that are not amenable to banding. 7
The two most commonly performed techniques are the conventional excisional haemorrhoidectomy, in which the haemorrhoidal tissue is excised and the wounds left open or closed, and the stapled haemorrhoidopexy, in which a circular stapling device is used to excise a ring of redundant mucosa and reposition the haemorrhoidal tissue within the anal canal. 8
Both surgical approaches produce excellent long-term outcomes in terms of symptom resolution and recurrence rates, but both carry a recovery burden that is considerably greater than that associated with banding. Post-operative pain following conventional haemorrhoidectomy is well documented as one of the most significant barriers to patient acceptance of surgical treatment, with pain during defecation in the weeks following surgery frequently described as severe despite adequate analgesia. 9
A trial published in Diseases of the Colon and Rectum found that patients undergoing conventional haemorrhoidectomy reported significantly higher pain scores in the first two weeks following surgery, required significantly more analgesia and took significantly longer to return to normal activity compared with those treated with banding, despite achieving higher long-term cure rates. 10
The key consideration in choosing between the two approaches lies in balancing the greater efficacy of surgery against its more significant recovery burden. Stapled haemorrhoidopexy is associated with higher rates of long-term recurrence and a small but recognised risk of serious complications. This has led to updated NICE guidance recommending that patients be fully counselled about these risks before undergoing the procedure. 11
How the Evidence Compares
The comparative evidence base for haemorrhoid RBL versus surgical haemorrhoidectomy is extensive and provides clear guidance for clinical decision-making across the different grades of haemorrhoidal disease. For grade one and grade two haemorrhoids, RBL is consistently demonstrated to be the superior treatment choice, offering symptom resolution rates comparable to surgery with significantly lower complication rates, no requirement for anaesthetic and a dramatically shorter recovery period. 2,6
There is no clinical justification for proceeding directly to surgery for haemorrhoids of this grade in the absence of a specific contraindication to banding. For grade three haemorrhoids, the evidence supports RBL as the appropriate first-line intervention, with surgery reserved for cases where banding has failed to achieve adequate symptom control after an appropriate course of treatment. 12
A Cochrane review examining treatments for haemorrhoids found that RBL was more effective than injection sclerotherapy and comparable to haemorrhoidectomy for grade two and grade three haemorrhoids in terms of symptom resolution, while producing significantly fewer complications and a significantly better patient experience. 13
As well as this, a large prospective study published in Gut found that 77% of those treated with banding achieved complete and sustained symptom resolution without requiring further intervention, with the remaining patients either requiring repeat banding or proceeding to surgery. 14
These figures support RBL as a highly effective first-line treatment that spares the majority of patients from the need for surgical intervention altogether. For grade four haemorrhoids, which are permanently prolapsed and irreducible, surgical haemorrhoidectomy is the appropriate treatment, as RBL cannot achieve adequate tissue reduction in this setting. 4,7
Why Patients Prefer Banding
Beyond the clinical evidence, the patient experience of haemorrhoid RBL compared with surgical intervention reflects a consistent and clear preference for the minimally invasive approach among those who have experienced both or who are making a treatment decision. The absence of anaesthetic is a significant factor for many patients, as the prospect of general anaesthetic carries its own anxieties for some people.
For example, there are the logistical implications of a procedure requiring anaesthetic, including fasting, escort arrangements and the recovery period from anaesthesia itself, which add to the overall burden of surgical treatment in ways that banding entirely avoids. Recovery time is perhaps the most decisive factor. Most patients treated with haemorrhoid RBL return to work and normal activities within one to two days. 5,6
Patients undergoing haemorrhoidectomy typically require two to four weeks away from work, during which pain, hygiene management, and restricted activity significantly affect quality of life. 9,10
For people in physically demanding occupations, with caring responsibilities or with limited capacity to take extended time off work, this difference is not merely a matter of convenience but a practical determinant of whether treatment is feasible at all. The complication profile of banding is also considerably more favourable than that of surgery, as serious complications following RBL are rare, with the most significant being post-banding haemorrhage in approximately 1% of procedures. 15
This compares favourably with the complication profile of haemorrhoidectomy, which includes post-operative bleeding, urinary retention, infection, anal stenosis and the small but meaningful risk of faecal incontinence associated with any anal surgical procedure. 7,9
When Surgery Is the Right Choice
It is important to be clear that surgery remains the most appropriate treatment for a specific group of patients, and the preference for banding should not be interpreted as a universal recommendation against surgical intervention.
Surgical assessment and management may be appropriate in situations, such as:
- Grade four haemorrhoids
- Large symptomatic grade three haemorrhoids that have failed to respond adequately to banding
- Combined internal and external haemorrhoidal disease, where the external component is significantly symptomatic
- Haemorrhoids complicated by thrombosis, ulceration or significant skin tags. 4,7,12
A thorough clinical assessment is essential to ensure that the treatment recommended is matched to the individual’s anatomy, symptom burden and clinical circumstances rather than applied as a default.
Haemorrhoid Assessment and Treatment at The Health Suite Leicester
If haemorrhoids have been affecting your daily life and you have been putting off seeking help because of concerns about treatment, a specialist assessment will establish exactly what grade and type of haemorrhoids you have and which treatment is most appropriate for your individual circumstances.
If you have grades one to three, RBL may be right for you:
- Grade 1: bleed, no prolapse
- Grade 2: prolapse during bowel movement, reduces spontaneously
- Grade 3: prolapse, requires manual reduction.
At The Health Suite Leicester, our Consultant Colorectal Surgeons provide a thorough clinical assessment and the full range of haemorrhoid treatments, including outpatient rubber band ligation for suitable patients, in a discreet and professional setting.
Where banding is the appropriate treatment, this is performed as a straightforward outpatient procedure with no anaesthetic and a rapid return to normal activity. Where surgical management is indicated, we provide clear guidance on the options available and what each involves.
Haemorrhoids are a common, treatable condition. There is no reason to continue managing symptoms without help; RBL may offer a quick, low-risk option for you.
Find Relief from Haemorrhoids
Explore our haemorrhoid assessment and treatment at The Health Suite Leicester and find out how we can help you

Haemorrhoid Banding
Private Haemorrhoid Banding in Leicester. Non-surgical, consultant-led rubber band ligation to quickly shrink bleeding or prolapsing internal piles.

Haemorrhoid Removal
Private haemorrhoid clinic in Leicester. Discreet consultant-led consultations, grading, and rapid referral pathways for surgical removal.
References
Have a query about Haemorrhoid Banding vs Surgery: Why Patients Prefer Minimally Invasive Treatment?
We recognise that getting the healthcare assistance you need can be difficult. So if you have a query, feel free to contact us and one of our treatment co-ordinators will be happy to help. We aim to reply to all queries within 24 hours (Mon – Fri).